


Suffering hands in medieval Dutch communities
Osteoarthritis (OA) is the most common joint disease, affecting around 1.5 million Dutch people today (around 10% of adults). You may know of it as “arthritis”, or “artrose”, and it is a disease of the soft cushioning tissues that surround the ends of bones within certain types of joints.
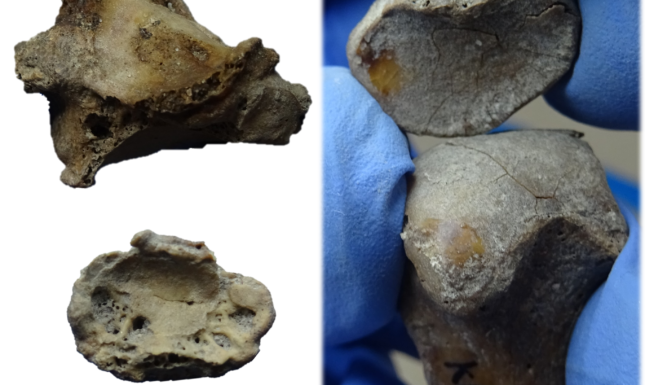
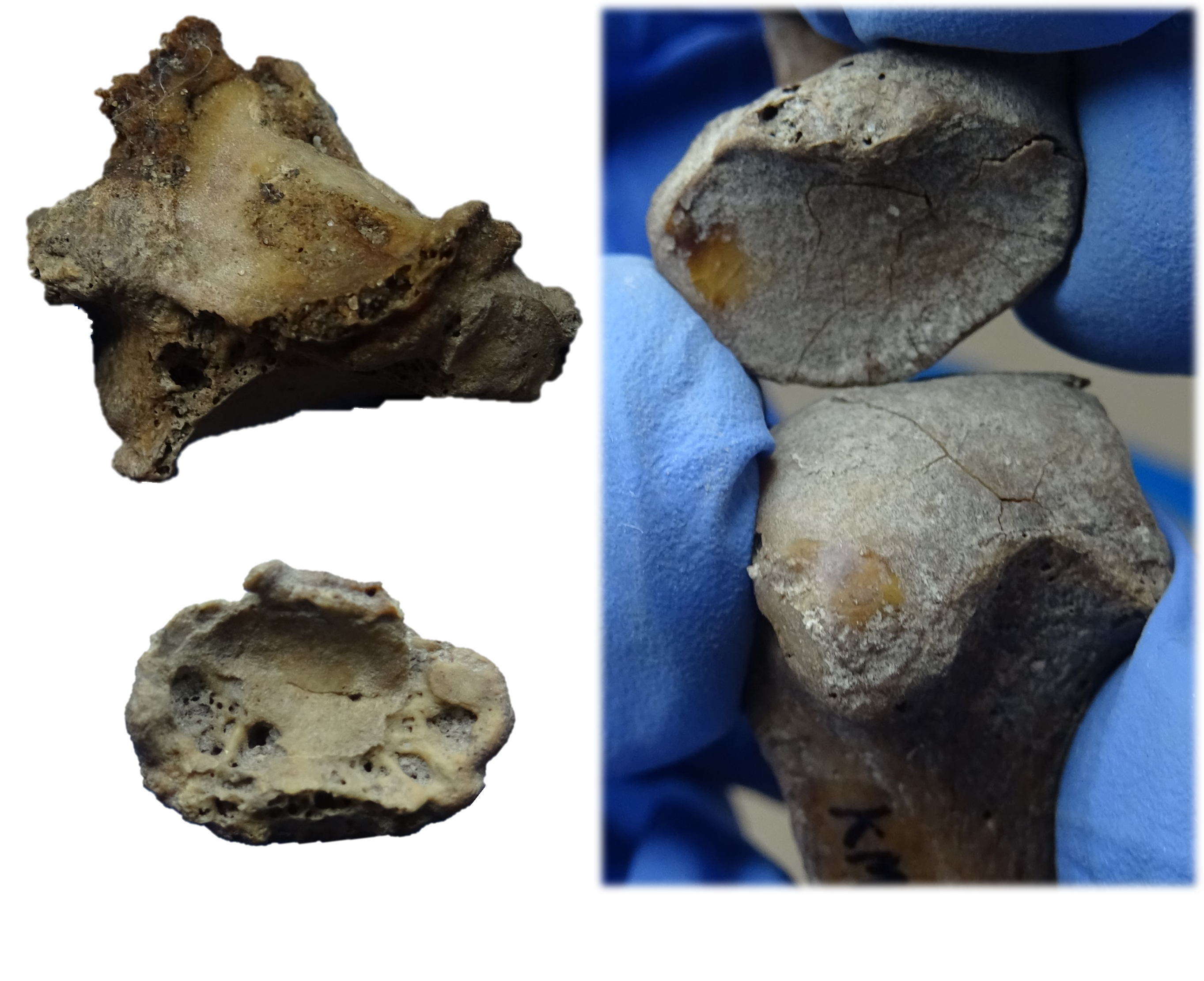
When this cushioning tissue breaks down, it slowly disappears causing predictable destruction, bone growth and polishing in and around the affected joints (fig. 1). This results in symptoms such as swelling, pain and discomfort, which in extreme cases can reduce mobility and overall hand function.
OA is considered an extremely complicated degenerative disease with no clear causative factor. Typically, it has been considered representative of the general “wear-and-tear” of our daily lives, causing the joints to wear down over time. However, modern medical researchers are skeptical of this, suggesting alternative causes such as aging, genetics, trauma, or strenuous/repetitive day-to-day physical activities. The causes for OA to develop happen to be of interest to osteoarchaeologists as well.
Skeletons and Osteoarthritis
OA is the most identified pathological condition we find when we analyse the bones of humans. It has been studied in archaeological populations as potential indicators of daily activities, but the focus is primarily on the larger joints; shoulders, elbows, hips, and knees. Hands, despite their daily use in our environmental interactions, have been understudied. We sought to investigate this a bit further, resulting in the first study of archaeological hand OA in the Netherlands.
Hand OA in the Medieval Netherlands
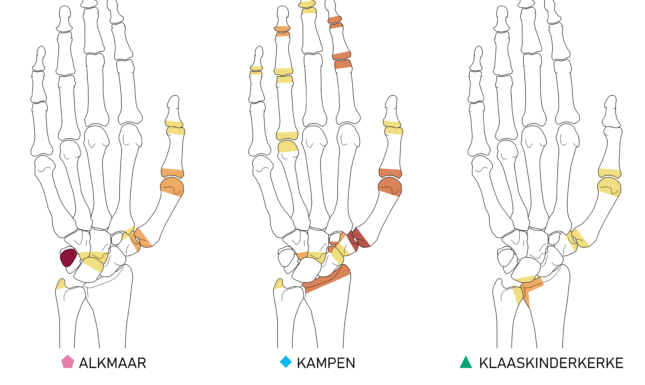
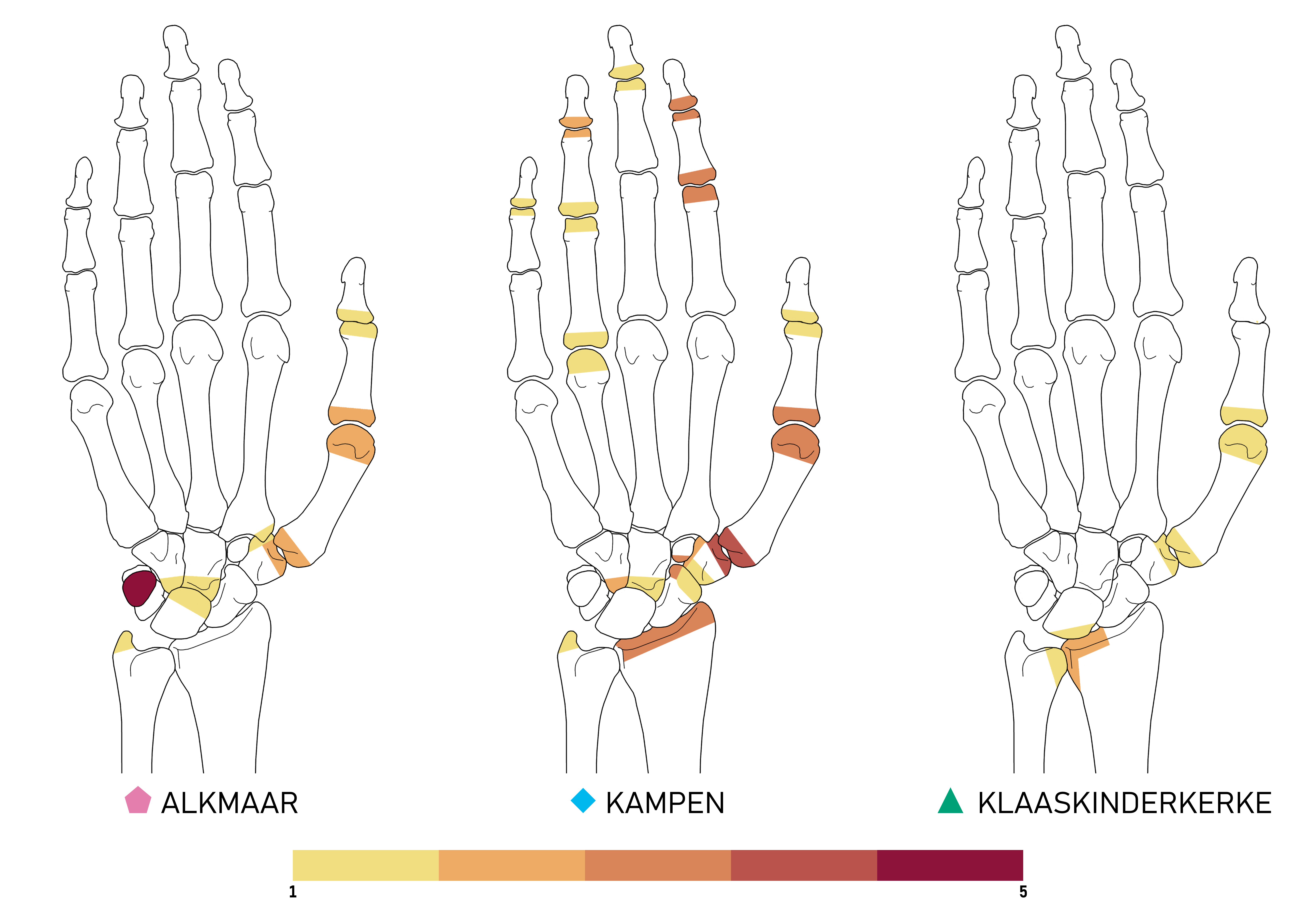
To explore OA in our hands in more detail, I analysed the hands and wrists of 224 medieval Dutch individuals from three different sites (fig. 2). The sites were selected due to the variation in their context; an urban population from Alkmaar (⬟), an urban hospital population from Kampen (◆), and a rural population from Klaaskinderkerke (▲).
In total, 16% of the analysed individuals had OA in at least one hand. This differed considerably per site, with Kampen showing the highest prevalence of 33%, then Alkmaar with 12%, and Klaaskinderkerke with 5%. This was an interesting find as these sites differ in environment, population status and daily activities/occupations. Most interestingly, the affected parts of the hands and wrists were not consistent between sites. There were considerable differences between the pattern of affected joints (fig. 3).


What's next?
Moving forward, we are going to explore these patterns in the context of the kinds of activities we might expect from these sites. Hopefully, this will help in determining whether the patterning differences have an activity-based origin, or whether this may be the result of genetics, or something else entirely. What is clear is the interesting difference between these three medieval sites, which warrants further exploration. Stay tuned for a future publication.
© Rachael A. Hall, 2023. Unauthorised use and/or duplication of the images presented in this blog, without express and written permission from the author, is strictly prohibited.



0 Comments